Degenerative Cervical Myelopathy (DCM)
Degenerative cervical myelopathy (DCM) is the most common cause of non-traumatic spinal cord dysfunction in adults. Precise assessment of clinical severity, cord signal change, focal vs multilevel compression, and sagittal alignment determines whether to approach anteriorly, posteriorly, or in a hybrid fashion.
Key Points
- Clinical: hand clumsiness, gait imbalance, long-tract signs, urinary urgency; use mJOA for severity.
- Imaging: MRI for canal compromise and intramedullary T2 hyperintensity; CT for OPLL and osteophytes.
- Alignment: lordosis vs kyphosis, K-line, focal ventral pathology vs multilevel dorsal compression.
- Surgery: ACDF/corpectomy for focal ventral disease; laminoplasty/laminectomy-fusion for multilevel disease depending on alignment and axial pain.
- Early surgery halts progression; degree and duration of myelopathy predict recovery.
Clinical and Exam
- Upper motor neuron signs below the lesion: hyperreflexia, Hoffmann, Babinski, clonus; wide-based gait.
- Hand dysfunction: loss of fine motor skills, myelopathic hand signs.
- Rule out mimics: B12 deficiency, ALS, peripheral neuropathy, syrinx.
Imaging Examples

Sagittal cervical MRI demonstrating degenerative changes. Source: Wikimedia Commons (CC BY-SA 3.0; © Stillwaterising).
{kind=link}

Compressive myelopathy at C6-C7 with T2 signal. Source: Wikimedia Commons (CC BY-SA 3.0; © Jmarchn).
{kind=link}

Upper limb dermatomes (anterior). Useful in correlating radicular pain distribution in concomitant radiculopathy. Source: Wikimedia Commons (Public Domain; Gray’s Anatomy plate 812).
{kind=link}

Upper limb dermatomes (posterior). Source: Wikimedia Commons (Public Domain; Gray’s Anatomy plate 813).
{kind=link}

Lower limb nerves. Included for completeness when assessing combined myelopathy and long-tract signs. Source: Wikimedia Commons (Public Domain; Gray’s Anatomy).
{kind=link}
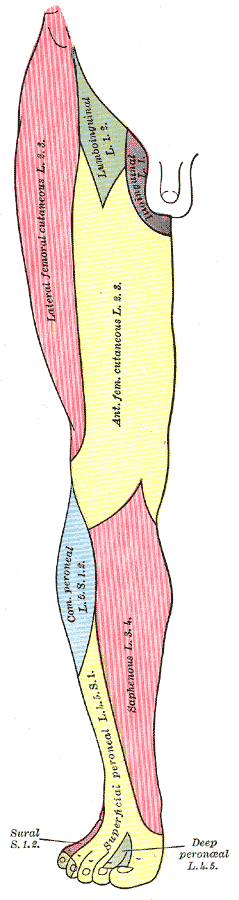
Lower limb dermatomes (anterior) to corroborate long-tract sensory changes. Source: Wikimedia Commons (Public Domain).
{kind=link}
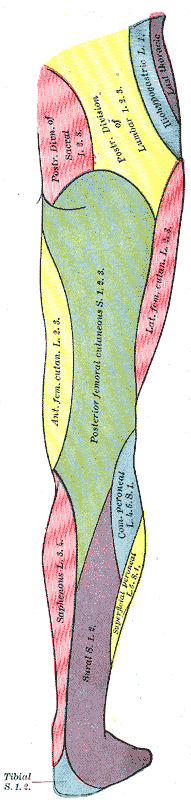
Lower limb dermatomes (posterior). Source: Wikimedia Commons (Public Domain).
{kind=link}
Surgical Strategy
- Anterior (1–2 levels, focal ventral pathology): ACDF for disc-osteophyte complex; corpectomy for retrovertebral compression.
- Posterior in preserved lordosis and multilevel disease: open or MIS laminoplasty vs laminectomy-fusion; choose fusion with axial pain/instability or kyphotic drift risk.
- Kyphosis or K-line negative OPLL: anterior or staged/hybrid correction.
- Pearls: preserve or restore lordosis; watch for C5 palsy risk with posterior decompression; evaluate dynamic factors on flexion-extension.
Outcomes and Counseling
- Early surgery halts deterioration and often improves gait/hand function.
- Worse prognosis with long symptom duration, severe pre-op deficit, and marked T2 hyperintensity with T1 hypointensity.
- Use standardized scales (mJOA, Nurick) for follow-up; emphasize fall prevention and rehab.
You can contact us at @bdthombre(https://www.linkedin.com/in/bdthombre/ ) on LinkedIn.